Thank you so much for being our special guest, and accepting this invitation for me to interview you for our ‘In conversation with’ series….what an honour! I was incredibly interested and excited to read about the subject you have chosen to study, as many years ago I worked as a consultant midwife, and one of my responsibilities was to support women to have the birth they wanted. I did this by working closely with women, and with midwives and obstetricians. Together we ‘pushed boundaries’ – which wasn’t easy, when ‘fear’ was (and still is) prevalent, and influenced the actions maternity care workers took on a daily basis.
So let’s here more!
I know you are studying for a Ph.D. at the moment, can you tell us about the topic have you chosen and why?
My current study centres on exploring midwives who actively choose to facilitate women’s unconventional birth choices whilst working within the NHS. By unconventional, I mean women’s choices that perhaps are outside of guidelines or where women decline recommended care. Largely, this topic has been born out of my previous Master’s research that explored why women choose to freebirth. The findings in that study demonstrated many unfortunate examples of poor midwifery care, namely around women feeling their choices were restricted and some even experienced coercive and threatening practices such as unnecessary referrals to social services. Listening to the women, whilst also being a practicing midwife with a range of experiences (good and bad), I wanted to turn my research questions around and to actively seek out the midwives who are managing to facilitate true woman-centred choice, as I know they exist! I am particularly interested in the midwives practising this way whilst facing the tensions that all maternity professionals face; busyness, poor staffing, guideline-centric care etc. I felt that by exploring the experiences of midwives’ who are managing to facilitate women’s unconventional birth choices, it can be used for other’s to learn from to benefit women’s experience of maternity services.
Are you allowed to tell me any of the preliminary findings at all?
I can tell you that recruitment was a great success! I had over 80 inquiries, and have recruited 45 midwives to the study. The midwives are from all over the UK, working in a range of roles; community, hospital, specialist roles and they also range from Band 5-Band 8. This is particularly useful going forward as all midwives working in any part of the service will benefit from the findings, as they will be relevant to a wide scope of practice. The midwives were invited to write an account and/or be interviewed so that together, we could explore practice stories of caring and facilitating women’s unconventional birth choices. This was to ascertain what the midwives do, how they do and also why they practise in that way. The birth choices women made were hugely varied such as; declining inductions, actively pursuing home birth or access to birth centres whilst with medical or obstetric conditions or declining certain observations during labour. Consistently, throughout the interviews was the importance of relationship building between the midwives and women, where open, honest conversations were central to the care planning and caregiving. It was interesting to note that some midwives worked in continuity models of care and others did not which is also useful as it helps us learn how to practice woman-centred care even when continuity is not available. As you can imagine, the scope of the findings will facilitate a wide range of knowledge generation to learn about complex midwifery practice. But for me, what has been so exciting and inspiring is hearing the commitment of the midwives’ to woman-centred care even in very unusual situations, something I think we can agree will help us move forward on the Human Rights in Childbirth agenda. That is all I can say for now, as data collection is still ongoing!
What are your personal thoughts about women choosing ‘unconventional’ births?
My personal thoughts about women making ‘unconventional’ birth decisions are that arguably many of the decisions shouldn’t be deemed ‘unconventional’ in the first place! If choice is a true choice, then it is reasonable to consider that a number of women will decline our suggestions or recommendations. Evidence suggests that women are sometimes steered into compliance which I feel is unacceptable, I firmly believe and am committed to women making their own autonomous decisions. Unfortunately, I feel a side effect of increased maternity surveillance, fear of litigation and the overuse of guidelines means that women are increasingly categorised into simplistic notions of high or low risk, which are not always helpful for either women or maternity professionals. By women pushing our ever narrowing boundaries in maternity care, they are teaching as valuable lessons in birth physiology and birth psychology.
What are your plans for the future?
What a tricky question! Well, I feel that my work is only just beginning and there will be many unanswered questions following this particular study which means continuing my research path. I am passionate about exploring ways we can learn from our colleagues to create virtuous cycles of improved midwifery practice and woman-centred care. I hope to establish some future collaborations with other midwives and researchers to drive this work and that of others forward. I endeavor to maintain clinical practice as I love working with women and their families, I just hope there are enough hours in a day!
Do you have any suggestions for related reading material or video links/websites?
I also have to mention the fabulous Birthrights, a particular source of inspiration.
And finally……If you had the power to change 3 things in maternity services, what would they be?
I would employ more staff to reduce the relentless workloads midwives face, that way they will be able to provide appropriate, timely and compassionate care to ALL women, and not be on the brink of burn out. I would introduce a no blame compensation scheme immediately, the fear of litigation has caused many unintended negative consequences. I would want midwives to have their rota’s at least three months in advance, midwives need and deserve to have a work-life balance, manage childcare and other family commitments. Valuing and looking after midwives is an essential component to improving women’s birthing experiences.
Midwife and PhD student Claire Feeley
Well Claire, I loved reading about the inspirational and courageous midwifery practice, and I feel sure there’ll be a great response to your very important study. Your findings will be particularly important as we move from statutory supervision of midwives, to the new Professional Midwifery Advocate role, as I believe ALL midwives will need encouragement and support to be true advocates for women, and to facilitate the choices they make, safely.
We are beginning a series of ‘Shining the light on…’ blog posts, a space for YOU to share your work or ideas, to tell others about your innovations in midwifery or maternity care.
Please let us know if you would like to be next! We’re waiting….
TODAY THE LIGHT IS SHINING ON … LAURA GODFREY-ISAACS!
We are delighted to share Laura’s work and interests with you, and information of an exciting event that will be well worth attending!
Laura is an artist, midwife and feminist academic and activist. She spent over twenty years in the arts, as a visual arts, feminist academic and creative producer. In 2016 she graduated as a midwife from King’s College London, and now works at King’s College Hospital, London.
Laura aspires to bring her knowledge and experience in the arts together with midwifery, to bring fresh interdisciplinary perspectives to inform education, practice and research. She is currently Research Associate with The Digital Institute for Early Parenthood, Ambassador for Proceate Projects and co-lead of the Health policy committee at The Women’s Equality Party.
‘I’m really excited to tell you about this up and coming event. I’m delighted too, as I am involved as an artist/midwifery advisor and speaker. Oxytocin – Birthing the World takes place at The Royal College of Art, and is organised by Procreate Project in collaboration with The Museum of Motherhood USA This is an international research and community event designed to encourage conversations and exchange between medical, midwifery, academic and art sectors with the aim of facilitating collaborations between them and increasing awareness of women’s rights, and their emotional, physical and cultural needs during pregnancy, labour and the postnatal period.
‘Becoming MILF’ Madison Young 2014
Before qualifying as a midwife in 2016, I spent over twenty years in the arts, as a visual artist, feminist academic and creative producer, and projects like this are enabling me to bring these different aspects of my life together. What excites me is the potential for the arts to inform and enrich midwifery – through an analysis of social constructs around women’s bodies, femininity and birth, by creating images and projects which can illuminate and extend representations and understandings of birth and as a tool for midwives to explore their own creativity and reflection.
‘Lactation Station’ Jess Dobkin 2006
The panel Midwifery, Art & Culture will include a group of midwives who represent some of the ways in which these issue are being explored as they all have a different connection, through their practice, with art and culture, which will be articulated through presentations and discussion. It’s great to be able to provide a platform to discuss a range of artistic and cultural strategies in midwifery with Ellie Durrant – Midwife Diaries & Secret Community of Midwives in the Making, Emily Maclean – midwife, journalist and social media editor, Nabila Fowles-Gutierrez – midwife, activist, mother of 3, female entrepreneur & musician and Claire Harbottle – Independent midwife, artist and director of Nativity Hub Leeds.
My introduction to the panel will build on recent conference presentations I have given at The Normal Labour & Birth Conference in Sydney 2016, MaMa Conference 2017, VIDM 2017 and the RCM Annual Conference, which look at depictions of ‘Birth in the media’ and representations of breasts and breastfeeding including brelfies (selflies of women breastfeeding). By looking at work about birth and breastfeeding, by artists and birth activists, in relation to depictions in the media and the wider culture it is possible to chart dominant cultural constructs which often limit and constrain women’s understanding of birth, and offer wider, more complex representations that open up meaning and connection and encourage women’s autonomy and agency in birth.
This event will be a fascinating interdisciplinary event, which I hope will encourage more cross-over between midwifery, art and culture and ultimately benefit those working to enhance and improve maternal experience: artists, midwives, birth workers and activists.
Details of Oxytocin – Birthing the World
Saturday 3rd June, 9.30am – 5.30pm, Royal College of Art Battersea, 1 Hester Road, SW11 4AN
Please let Laura know if you want any more information, and what you think of this fascinating and important work!
ALSO… if you want to receive snappy, topical information about midwifery and maternity care, sign up here to receive our Sunday Summaries right to your inbox. Boom.
Anna and I are keen to invite guests to post blogs on interesting topics. We also would like to ‘interview’ individuals who have made a difference, inspiring our profession from within or alongside. Do get in touch if you would like to be ‘In Conversation’ with us……
Here, is Julia!
Hello Julia, thank you so much for agreeing to this interview! Would you start by telling us a little bit about yourself? Just a little?
I was born in September 1939 at Greenwich, my father was already in France, I didn’t see him until I was six. I have two younger sisters and a brother. I was a grammar school girl. Barrie and I married in 1960 and had a boy and a girl. We lived in Australia for two years. We now have, seven grandchildren and 17 great-grandchildren. Our daughter and one of my sisters were also midwives.
I know you had a very successful midwifery career, when did you commence your training, and what were the highlights?
I applied to train in 1969, I was offered a place on the direct entry programme in Nottingham. My training and the time I spent on the district, with my teaching, district midwife Joyce, has informed everything I have done since. Once qualified, I worked as a district midwife, giving the one to one care at home, that few women or midwives get to experience today. District midwives worked alone, other than support from the woman’s family or friends. When home births dwindled, I trained as a midwife teacher. I gave my intention to practice independently to deliver my grandson at home. I read for a Masters in social policy and administration, at Nottingham University, England, and began the research which would eventually become ‘Delivered at Home’. I was appointed Head of Midwifery Studies at University of East Anglia. The Department of Health bought my time from the University to write an account of my research, this was given as evidence to the House of Commons Select Committee, which produced Changing Childbirth. Later I was appointed as President of The Royal College of Midwives (see photo below!) and then General Secretary.
Julia as President of the Royal College of Midwives, 1992
What do you think has changed between the midwifery you knew, and now?
Everything has changed, particularly the belief that childbirth is a normal process, which can mostly be safely managed by a mother and a midwife working together.The propaganda that birth is only normal in retrospect, damages the confidence of midwives and mothers. The loss of the Central Midwives Board (CMB), which, while it controlled midwives and their practice and protected childbearing women, it also understood, supported and encouraged the profession.
I love your book, ‘Delivered at Home’ – what inspired you to write it?
I was inspired by all the midwives and mothers who wanted, but would never experience a home birth. The last of the district midwives were the last midwives to have the courage of their convictions based on their own experiences. I was inspired by the fact that I knew home birth was safe, yet thousands of women every year were hospitalised for birth, against their wishes, using precious hospital resources unnecessarily.
Sheena says:this book is a ‘must read’ for anyone interested in the social history of childbirth and midwifery.
I see from Facebook that you collect midwifery memorabilia – which I find so interesting. Can you tell us about this hobby, and any special items of interest?
It began when I did the research for ‘Delivered at Home’. I collected some 200+ midwives’ registers from my colleagues to analyse. I still have some of them and others I have acquired along the way. I have a lot of CMB memorabilia and items given to me by Joyce, my district teaching midwife. I collect antiquarian books, especially related to midwifery. My favourite item is Joyce’s shorthand transcript, of an entire RCM refresher course, at Brighton c.1957, including midwives Q and As, at the end of each session. I am slowly transcribing it, Mr Fenny of the CMB gave one of the presentations.
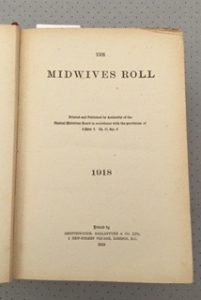
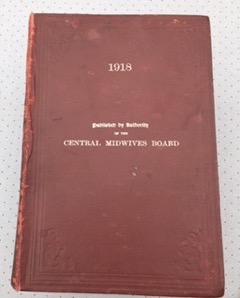
Julia sent photographs of the artifacts above (left to right) 1918, CMB Roll of Practising Midwives, showing cover and front page, and the badge of E. Harper, roll number 44410, who qualified on 26.6.1916.
What are your plans for the future Julia?
I am determined to reveal the historic outcomes of midwifery care, before the arrival of accoucheurs. Most existing histories would have us believe that maternal and infant mortality was very high before medical men intervened. I have tested this theory, by searching Tudor records, finding midwives and analysing their birth outcomes. I transcribed six 16th century parish registers, from Latin or English. I was awarded a PhD and an Hon. DSc. in 2013. I am now, transcribing the thesis into book form.
What gold nuggets of advice would you offer student midwives today?
You will be standing on the shoulders of some brave and wonderful midwives, Agnodice, Jane Sharp, Zepherina Veitch, Rosalind Paget, Catharina Schrader, Elizabeth Peverel to name a few. Believe in yourself, and believe in the women you care for. The measure of a true profession is its academic ability to explain its unique value to society. Midwifery has found a place in higher education and we must use the opportunities it offers to the full.
Letter from the RCM
Wow, Julia. Thank you so much for sharing a snippet of your life, your work and studies, and your fascinating hobby! You have left us hungry to hear more…we hope you’ll keep adding to this blog post, as you reveal other treasures.
Readers! Please leave your comments below, and tell Julia what you think!
Indie’s message to the world, for International Day of the Midwife 2017
Indie Kaur is a consultant midwife at the Royal London Hospital, and is currently on sabbatical working in Hyderabad, India, at the Fernandez Hospital. This hospital is owned by the inspirational obstetrician, Evita Fernandez, who is working tirelessly to develop professional midwifery programmes in her region. More about Evita, and her campaign, below!
We keep in touch with Indie, and recently saw this post on Facebook. We asked her if I could repost an adapted version of her words here, as we are in awe of the work she is doing, and the ground-breaking progress taking place in India.
It is now April in India.
I have been here for 3 months now. I must admit I love the sunshine despite this intense heat. All this sun, yet Indian mothers seem to be vitamin D deficient. The weather fluctuates between 33 to 42 C. I am on a journey, which is exciting, as I believe it will be a slice towards influencing professional midwifery services in India. But it is also frustrating. I am a professional midwife with over two decades of experience. However, I am unable to practice in this country due to the complexities and bureaucracy within the government, which by the way does not accept midwifery as a separate unique profession. Accountability within one’s sphere of practice therefore, is not accomplished.
It was the 1902 Midwives Act, which introduced training and supervision for midwives in England and Wales, outlawing uncertified and untrained (bona fide) midwives. However this legislation didn’t eliminate traditional birth attendants, as fewer midwives were available in rural areas. After 1910, all women were expected to have a qualified medical practitioner in attendance at the birth of their baby. Uncertified midwives were forbidden to attend women in childbirth without the direction/supervision of a medical practitioner. The newly registered midwives were initially required to have a 3 months training, which increased to six months in 1916 and a year in 1926, with the model of calling the doctor in difficult cases. The proportion of births attended by qualified midwives increased steadily and by 1930’s is almost all practicing midwives had received training and continues to have legislation changed. Today in the UK direct entry midwifery is a three year programme, and for registered general nurses it’s eighteen months.
Human rights violations
There are some similarities in India today to the 1920’s in the U.K. There are traditional birth attendants in rural India, and no professional midwives based on the International Confederation of Midwives (ICM) core standards. In the public institutions where the majority of women give birth, there are masses of vulnerable women, birthing in appalling desensitized environments. There is lack of dignity, respect and there are violations of basic human rights like privacy. They are cared for by health care professionals who are a mix of nurses, unskilled birth attendants (dais) and auxiliary nurses (erroneously called midwives) who lack the knowledge and training. The challenge lies in India urgently recognizing the need for professional midwives.
Evidence and choice
The place in which majority of women give birth in the UK has changed considerably over 100 years; following the Peel Report in 1970 birth went from home, to maternity institutions – hospitals. The Changing Childbirth Report in 1993 suggested that women should have a range of options of place of birth. The philosophy behind birth centres in the U.K is the provision of a safe environment for healthy women to give birth in outside the hospital, where the medical interventionist model dominates. The Birthplace Study in England clearly highlighted that healthy women, who gave birth in a midwifery led unit (MLU) had significantly fewer interventions, including substantially fewer intrapartum caesarean sections. The study also demonstrated that for healthy women, giving birth in a midwifery unit was as safe as hospital, for her and her baby. This gives women choice in place of birth, and allows doctors to focus on medical complications.
In the UK, MLUs (also called birth centres) continue to be sustained because there is a midwifery profession which is autonomous and accountable, and has been embedded into the healthcare system for more than a hundred years. However, in India, there are some birth centres run by midwives certified from overseas to help a rising tide of women demanding midwifery led support during their birth. Would it not benefit all childbearing women in India, to have a baseline cadre of professional midwives? Why does the government and the Indian Nursing Council not accept midwifery as a separate autonomous profession?
Visionary leadership
I am working in a tertiary referral perinatal center, with over 8000 deliveries per annum, providing clinical leadership to our midwives in the antenatal and intrapartum areas of care. I am lucky to work with a visionary leader Evita Fernandez an obstetrician, who understands the value of professional midwifery and how it can influence maternity care including reducing the mortality and morbidity rates in India. She launched an in-house professional midwifery education and training (PMET) programme in August 2011. Had she waited for bureaucratic approval, we would not have the rich data we have collated over the years of the impact of professional midwifery support on birthing experiences and outcomes.
Our professional midwives in Fernandez following our ‘train the trainer workshop’ conducted last year have recently trained health care professionals in the rural districts. We travelled to Nandyal (300 km) in April and four of our midwives trained health care professionals in obstetric emergencies drills of shoulder dystocia, pre-eclampsia, postpartum haemorrhage and neonatal resuscitation. The workshops were well received and the positive feedback from the participants was very encouraging. The medical director of the hospital that hosted this workshop, that very night, had a case of eclampsia, which was dealt with efficiently by the nursing team who had attended the workshop. A mother’s life was saved and long-term morbidity averted.
My friends – this is going to change outcomes and indirectly save lives of mothers in India.
Unlearning poor practice
Recently in Fernandez, the midwives experienced a Lotus Birth, as one of the mothers opted for this experience. The concept of listening to mothers and supporting them through their birth choices was strongly demonstrated with this mother’s request. The mother experienced lots of telephone calls from her family and friends constantly asking if she had had her baby. I was her point of contact and she felt assured with a daily phone conversation. When she came in spontaneous labor the midwife who had helped her birth her first baby was also available. This made the woman more happy and added to her comfort and feeling of safety. The midwives in Fernandez are learning to understand women and “unlearning” the need for repeated vaginal examinations. They are discovering the value of spending time with women, watching and listening while they understand the signs of progress of labour, without a vaginal examination. The mother raised the question of having a vaginal examination. She was comfortable and relaxed when we said ‘No’ and encouraged her to mobilize. She was relieved and had planned a water birth. The lights were dimmed and the clock on the wall turned off. When she relaxed, her contractions picked up after she had her supper and her older child slept. Her waters broke spontaneously, the intensity of her contractions increased, and she was ready to use the birthing pool. The cephalic pole was 2/5th’s palpable on abdominal palpation. She was four cms dilated with a thin well-applied cervix. She entered the pool and as she submerged into the water, she sighed with relief. The room was silent and her husband supported her with fluids. The midwife listened to the fetal heart and was completely in awe. This was a first water birth experience for her and the mother.
The environment was surreal and she chanted her mantra, adding a spiritual dimension to her labour. She birthed her baby in water just after midnight. The baby was brought up to her, took his first breath and cuddled up to his mother. Her placenta soon birthed and we kept it with her in a bag rubbed with rock salt and ”tulsi” which is an Indian herb with medicinal effect. This was also very rewarding for me. In my role as a consultant midwife in London, I have been steered into a managerial role. This “hands-on” clinical exposure filled me with deep satisfaction. I realized then how much I missed the clinical involvement and the rapport midwives develop with the women they help birth.
Midwife Jyothi Rapelli showing positions in labour to a mother
On the road!
The road trips in India are exciting. One encounters a variety of challenges- from a mix of good and bad roads, with cows and goats crossing over. Evita and I travelled 575 kms to The Krishna Institute in Karad, Maharashtra. I contributed to the driving under Evita’s beady eye, who in the passenger seat (obviously NOT her favourite position) ensured I learnt the rules of driving in India! I had to endure comments such as “This is India where majority of drivers do not stay in their lanes and do not warn you either when they cross. So watch out and yes- please hoot” The horn was used often enough to warn the driver ahead that I was going to overtake him….and yes, I was also reminded – ”You do not overtake two vehicles at a go”. Despite this, we survived the drive and arrived in the small university town. The hosting team was amazed and impressed that two women drove all the way themselves. We were treated as minor celebrities! On our arrival, we visited the labour and delivery wards. We were impressed with the efforts the team was trying to make, to improve the environment of birth. The workshop on Respectful Maternity Care was initiated under the Safe Motherhood Initiative, a programme spearheaded by the Dean of Nursing Studies. The next day, was spent in a think tank session to discuss practical action plans with time lines. Evita presented on birth experience and Human Rights in Childbirth, which is an urgent need for India. I highlighted the role of a professional midwife and her impact in supporting mothers, advocating and evidence behind positions in labour.
Evita Fernandez speaking to the trainee midwives
The success of this workshop lies with the conviction of Evita as an obstetrician endorsing the need for professional midwifery in India. We complimented each other’s roles. I shared my experience as a professional midwife in the UK, and now in Fernandez working under my sphere of professional accountability. We emphasized the strict need to adhere to the core clinical competencies as endorsed by the ICM. We both shared the challenges of working with a multi-disciplinary team and how it was worth every effort to work with protocols. We emphasized the need for drills and for doctors and nurses to work with respect for each other’s professional roles. All of this is needed if we wish to offer woman centered care in a high volume setting, such as their hospital, which has a 350 delivery rate every month.
I am now back in Hyderabad and attended my first Indian wedding. I was fortunate to have a personal dresser within our team with her immaculate dress sense, draped me in my sari. I felt elegant, sophisticated and stood tall at the reception. The hospitality and rich culture is amazing and the work reaps rewards. I can see the change evolving with the team. It is an ongoing journey and the decision to be a role model in India for a year has been the right path for me.
I shall keep you posted soon.
PLEASE READ ON…..
Dr Evita Fernandez campaign for professional midwives can be found here Professional Midwifery Services PROMISE – please donate to the cause if you feel able. Below is a link to an article by Evita, and an award winning video explaining more about the need for professional midwives.
We are delighted to welcome you to our very first blog post, on our brand spanking new website! We are launching our site today, on the International Day of the Midwife, to show our firm commitment to midwifery, to partnership and collaboration, and to spreading kindness and compassion for respectful, safe maternity care throughout the world.
Every year on the 5th May, midwives around the world celebrate, and are celebrated. In the UK, we are fortunate to have one of the best professional midwifery systems in the world. Though it’s far from perfect, we know there are countries where there are no midwives, or where midwives are constrained in their practice and unable to provide evidence based, sensitive midwifery care. The Lancet Midwifery Series, and the State of the World’s Midwifery Report provide the detail for us to see that the vast majority of maternal and newborn mortalities and morbidities in middle and low-income countries could have been prevented with proper antenatal care and the presence of a skilled midwife during birth.
Sheena with newborn Anna, grateful for the midwives who cared for them!